
The Madison-Area chapter of the Democratic Socialists of America condemns the public execution of George Floyd at the hands of the Minneapolis police. We stand in solidarity with protesters calling out the deeply entrenched pattern of violence, anti-Blackness, and oppression upheld by police in our country, in our state, and in our city. MADSA supports the entirety of last weekend’s demonstrations against the brutal police murders of George Floyd, Tony Robinson, Breonna Taylor, Tony McDade, Sean Reed, and countless others. Furthermore, MADSA calls upon elected officials who supported the Saturday afternoon march to follow through on that support by meeting the demands of its organizers, Urban Triage, Freedom, Inc., and the Party for Socialism and Liberation–Madison: defund the police, institute reparations for all Black people, release all incarcerated Black people from jail, get cops out of schools, and institute community control over the police. MADSA encourages financially supporting Urban Triage, Freedom, Inc., and the Free the 350 bail fund.
Tag: Feat-Apr20
-

Centering Workers in Economic Relief
Restaurant Workers Coalition Responds to Small Business Support Grant Program
A statement from the newly-formed Restaurant Workers Coalition. To support their work, please sign this petition and spread the word.
On May 3rd, Dane County Executive Joe Parisi announced a plan to direct $10 million in federal aid to small businesses, tasking the non-profit Dane Buy Local with operating a fund to disburse the money in the form of grants to local businesses. The Dane County Board of Supervisors will vote on the proposed allocation of grants on Thursday, May 7th. In the initial press release, Parisi did not offer specifics around oversight of the fund, and Dane Buy Local has not publicly specified how recipients would be required to use their awarded grant money.
The Restaurant Workers Coalition (RWC) is a Madison-based group of service industry workers organizing and advocating for workers’ material needs during the pandemic and after. RWC believes that it is vital that any economic assistance benefits workers directly.
“A lot of [us are] temporarily unemployed people. . . people who have had to quit due to safety concerns, people who don’t have sick time or who don’t have any sort of protections during this time,” says Lillian Myrhe, a restaurant worker in Madison and a member of RWC.
To meet the needs of not only workers in food service but those across industries, we ask that Dane County set specific guidelines around these funds to ensure that they are used for payroll and to provide PPE and hazard wages to workers on the floor.
Further, Dane Buy Local must follow through with all grant recipients to ensure that funds are allocated in the ways indicated in their grant applications. Finally, Dane Buy Local should be transparent about the distribution of grants, including the full list of successful applicants and a record of the reasoning behind their respective allocations.
RWC believes the Dane County Treasurer should establish a separate fund for direct allocation of resources to workers most impacted by the pandemic, particularly those who cannot access federal funds due to immigration or citizenship status. To learn more about RWC or to get involved, connect with us on Facebook or Instagram at Restaurant Workers Coalition, or email us at restaurantworkerscoalition@gmail.com.
-
Learning from Viet Nam’s Response to COVID-19
By Mary Croy
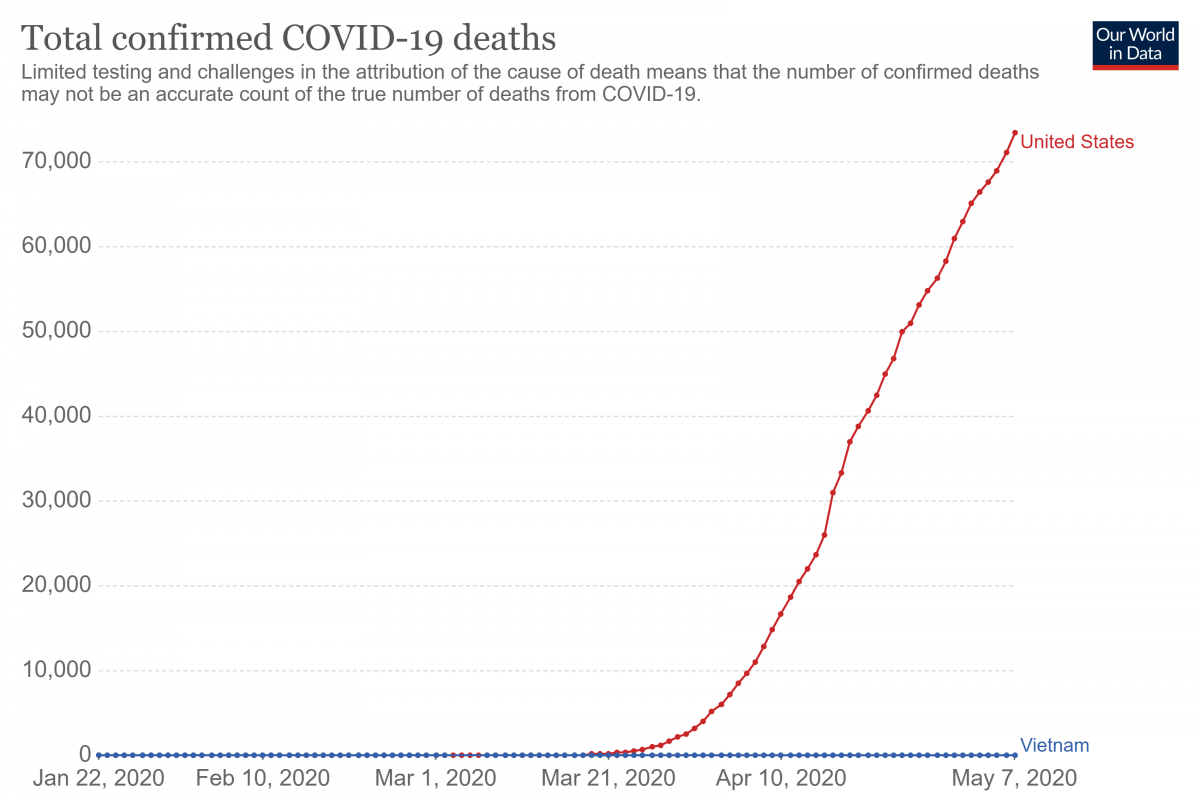
Viet Nam is a small country with a large population of 97 million people. Yet as of mid-April, there were 262 reported cases of COVID-19 and 0 reported fatalities. How can a developing country outperform the USA and all of Europe in defeating a deadly virus?
- Early action: As soon as the virus emerged in Wuhan, Viet Nam strengthened its border monitoring. Without banning travelers, officials conducted checks at airports and at the border for anyone exhibiting the symptoms of COVID-19. Those who had symptoms were isolated and monitored at the hospital.
- Viet Nam quickly instituted residential quarantine. Vinh Phuc town, a manufacturing center north of Ha Noi, was quarantined for three weeks. But quarantine in Viet Nam is different from quarantine in the US. People living under quarantine are given social support, such as a box of food delivered to every family in the area.
- Testing: Viet Nam quickly developed their own test kits and manufactured them domestically. In addition, they used contact tracing to track down and test the contacts of infected people.
- Medical students as well as retired health professionals have been brought into the fight. They have created cell phone apps to find out about hotspots and to ask for donations from those able to afford it.
- Viet Nam has transformed its manufacturing base into an engine to produce equipment needed to fight the virus. 450,000 protective suits have been donated to the U.S. and 550,000 masks were sent to Europe.
As socialists, we can learn some lessons from the Socialist Republic of Viet Nam. Control of production and the ability to quickly manufacture needed equipment is a crucial part of protecting public health.
Mary E. Croy lived and worked for nine years in Ha Noi, Viet Nam
-

Rejecting Eco-Fascist Ideas Arising from the Pandemic
By Ben Heili
Eco-fascism thrives on memes. You’ve likely seen this one: In the middle of pandemic-related social distancing and shutdowns, nature returns to an area previously dominated by humanity, from Venice to Los Angeles to suburbia. After a few serious posts, internet humorists created joke versions of the meme, featuring over-the-top exaggerations like a picture of pink and purple Lisa Frank-designed dolphins “returning” to the Hudson River. The meme’s formula ends with the words “We are the virus.” This is a dangerous and misplaced idea that echoes many genocidal campaigns of the past. In fact, many versions of this meme have been used to poke fun at the macabre thesis. But the past few years have shown it can be dangerous to play with fascistic themes even on an ironic basis. Far-right groups are consciously using online communities driven by irony and cynicism to bring frustrated young men further and further toward their hateful message.
This mixture of fascism, a tongue-in-cheek stance, and ecology was most visible in the actions of the Christchurch mosque shooter last year. He put together a multimedia manifesto including a grisly livestream, and throughout his message were strong strains of both hatred and a
twisted, internet-based form of humor. One of his claims, seemingly not a joke, was that the environment was being wrecked and that non-white outsiders were to blame. “If we get rid of enough people, then our way of life can be more sustainable.” This is the core of modern eco-fascism. It is a correct recognition that humanity’s current way of living is destroying its only home, then a horrifying proposal that aligns with pre-existing racist ideas about who is deserving, who is human, and who must die.
We have not yet seen many explicitly eco-fascist ideas implemented by governments, but we already know that the impacts of both COVID-19 and climate change are distributed unequally along the lines of race and class. While denying the obvious about global warming and mass extinction, the Trump administration weaponizes its effects against political and racial enemies. With the incompetent and callous response to Hurricane Maria, we saw a preview of his stance. He considered Puerto Ricans less-than, and refused to support their rescue and recovery. Now, the administration withholds aid shipments from states or personalities he considers political rivals, and the structures of our society make the virus more deadly for the incarcerated and for already oppressed minority populations. As long as the Repubican Party maintains its deadly embrace with the fossil fuel industry, it is not likely it will outright embrace eco-fascism, which acknowledges man-made climate change. But it can leverage ecological disaster to further dispossess everyone but its wealthy donors.
The eco-fascism seen in COVID-19 memes is mild in comparison to these examples, yet it mimics the pattern seen elsewhere. The response to the issue lies in a culling of humanity, not a change in humanity’s production and consumption. Some of the most successful movies of the past decade, the Avengers series, centered around a villain who wanted to wipe out half of all life in the universe for purposes that mirror real-life eco-fascism. A Reddit community called “Thanos Did Nothing Wrong” gained over half a million subscribers. Again, most participated ironically, but it was a perfect way for online fascists to blur the lines between extermination rhetoric and popular American culture.
Anyone who believes in shared human rights must reject the eco-fascists’ conclusions… Humans are not the virus. It is capitalism that pushes us to exceed earth’s capacity, to produce for the sake of production.
Anyone who believes in shared human rights must reject the eco-fascists’ conclusions. Humanity has the capacity to map out, plan, and consciously balance our relationships to all other species and to the earth’s resources. It will take effort and ingenuity to do so, and more to undo the harms that push earth’s species toward extinction. But it is not impossible.
Humans are not the virus. It is capitalism that pushes us to exceed earth’s capacity, to produce for the sake of production. Killing people or letting people die in disasters like the COVID-19 pandemic will not solve the climate crisis, and we must not crush and loot our planet’s diversity to serve this machine. The only just way forward is through organization, technology, refocusing our presence to accomodate the needs of all species, and controlling the damage we have done so far.
-
I’m Using My Stimulus Check to Pay For An Abortion
Shared Anonymously
I am using my stimulus check to pay for an abortion.
As I went from Day 35 with no period, to Day 36, 37, 38, I thought seriously about what to do if this wasn’t just a late period. It became very clear that getting an abortion was the right choice for me, my husband, and my family in this moment. We have a 15-month-old and we want a second kid, but the thought of a pregnancy, a birth, and a second baby amid a pandemic – when we could lose our jobs, when a hospital delivery could be dangerous and isolating, when our out-of-state and elderly parents couldn’t travel to help in those early weeks of parenthood – is terrifying. In fact, were it not for the pandemic, we very well could have made a different decision. As Republican governors across the country question whether abortion is an essential service in these times, I know it absolutely is—all the more so because of these times.
Though we made this decision quickly, my husband and I didn’t make it lightly. It didn’t take long for other thoughts to creep in. I felt dumb for getting pregnant: I miscarried two years ago after trying to conceive for a year, and I have a toddler. I know exactly how this works. I felt shame for making this decision: isn’t this a frivolous reason to do something so serious? Aren’t abortions reserved for when you really need it? Of course, my internalized guilt couldn’t specify who should get to determine justified need. Will people I love hate me? That wasn’t even a question, because I knew at least some would. The real question was whether they knew they hated me specifically when they spoke in generalities about the sanctity of life and abortion as murder. Is this the burden that people I love who have had abortions have carried with them for decades?
How dare this society make women hate our bodies, make us want to hide them away, perfectly priming me to think I don’t even deserve to control mine?
As I type this, I hear my husband on the phone with his mom. She loves us and supports us, and also has concerns about the burden of going through with this. Is this how stigma creeps into relationships? Wedging itself, word by loaded word, into conversations? Creating silence and one-word responses where there should be jokes and laughter?
Also while writing this, I bought myself a swimsuit for Mother’s Day (“for” is generous, quite frankly, that just happened to be the nearest excuse on the calendar for retail therapy). As a mother I am more in awe of my body than ever before. I’ve always hated most of it; on a good day, only parts of it. But my body is amazing. It creates life, it nourishes life, and somehow it keeps me going, too. How dare this society make women hate our bodies, make us want to hide them away, perfectly priming me to think I don’t even deserve to control mine?
Before moving to Madison I lived in Washington, DC and volunteered as a clinic defense escort at a Planned Parenthood just a few blocks from the White House. I saw Catholics pray in circles in front of the clinic. I witnessed white Anti-choicers harass Black patients with race-baiting arguments. For years, I heard dehumanizing hate spewed along the clinic sidewalk week after week after week.
Last week, when I arrived at Madison’s East Side Planned Parenthood, I saw a lone old white man wearing a sandwich board that explained contraception as “chemical pornography.” Of all his slogans, that one was actually the most logical; the others I couldn’t make enough sense of to remember. He yelled when I got out of my car, lazily, in my general direction. I was already frustrated by the fact that I couldn’t exercise basic autonomy over my body in this moment – by the fact that I had to be treated like a child, forced to wait a week to make sure there were no take-backs – and I was in no mood for this harassment. I stared him down and yelled “Sir you can go straight to hell.” This time, he acknowledged me directly and yelled back: “You think you’ve changed my mind but you haven’t.” I don’t think he got the irony of the moment. I told him “Right back at you,” but I still think it went over his head. When I left the clinic two hours later, he was still there, joined now by an old white woman saying the rosary. I flipped both of them off as I drove home.
Inside the clinic, the staff was kind, compassionate, and respectful. I was there just for a consultation. Due to a 1996 law I have to wait 24 hours before actually having an abortion. Due to a 2012 law I have to be seen by the same doctor for my consultation and abortion, and because of limited staffing (no doubt due to ideologically-driven funding cuts) that meant the 24-hour waiting period would be a full week.
During my consultation, a staff person explained the process of a medicated abortion. First, I would take a pill called mifepristone to block hormones from reaching the small, almost invisible cluster of cells inside my uterus (thanks to a 2013 law she was forced to conduct an ultrasound of this cluster of cells and show it to me, though I was not obligated to look. I looked anyway; the flowery covering on the overhead fluorescent light I was staring blankly at made me feel pitied, and I did not want to be pitied.). Then, I would take a pill called misoprostol to tell my uterus to contract and expel those cells.
In February 2018, I underwent almost the exact same thing after learning that a pregnancy I desperately wanted had stopped developing at 9 weeks. It was heartbreaking and traumatic, and the physical and emotional memory of that moment will stay with me forever. At the time of my miscarriage, pharmacists from Michigan to Arizona were denying misoprostol for women suffering from the trauma of miscarriage because it is used in abortion. In my consultation, the staff person told me doctors here are also having trouble prescribing mifepristone for other uses because of its link to abortion.
Mothers know the physical burden of parenting: our bodies are not our own for 9 months as they are sapped and stretched to grow a little human.We know the emotional and mental burden of setting aside every other pressure in life to take care of this vulnerable, frustrating, perfect little one we’ve brought into the world. We know the financial burden of simply trying to survive.
Because I had taken misoprostol before, and because surgical abortion can be more than twice as expensive, I opted for the medicated abortion. My insurer stopped covering abortion years ago, so my costs would be out of pocket. My only concern was whether the prescriptions would affect breastfeeding; it’s a question you get used to asking as a nursing mom. The staff person told me it was a common question to ask. Let that sink in for a moment: people seeking abortions commonly ask if the medication they will need to take will interact with breastfeeding, because they already have small children at home.
Mothers know the physical burden of parenting: our bodies are not our own for 9 months as they are sapped and stretched to grow a little human; add another 6 months, or year, or more onto that if you nurse your baby. We know the emotional and mental burden of setting aside every other pressure in life to take care of this vulnerable, frustrating, perfect little one we’ve brought into the world. We know the financial burden of simply trying to survive; daycare costs more than my mortgage, and in Madison we were fortunate to even find an opening when we needed one.
At the end of my consultation, I met with the doctor who would prescribe my medicated abortion. She was legally required to read a two-and-a-half page document to me, telling me such things as:
- “The numerical odds of survival for an unborn child delivered at that probable gestational age.” Zero percent.
- “The probable anatomical and physiological characteristics of the fetus on this date.” Literally none. At just over 5 weeks, I had an embryo inside me, not a fetus, and my mandatory ultrasound showed a gestational sac that even to a trained eye looked empty.
- “The medical risks associated with the particular abortion procedure that would be used, including the risk of infection, psychological trauma, hemorrhage, endometritis, perforated uterus, incomplete abortion, failed abortion, or danger to subsequent pregnancies and infertility.” I am more worried about the actual trauma of pregnancy and childbirth in COVID than the feigned concern of anti-choice zealots.
- “That no payment for the procedure may be required from me until at least 24 hours have elapsed after the informed consent consultation has been completed, except if the waiting period is shortened by me because the pregnancy is the result of sexual assult or incest or medical emergency.” What must it be like to pass through the world with a body whose autonomy is not conditional? With a body that demands respect and trust wherever it goes, whatever it does?
- “A list of providers that would perform the required ultrasound at no cost to me.” Conveniently, there’s a very pink “crisis pregnancy center” just across the street from Planned Parenthood that I’m sure would be thrilled to talk to me. Unfortunately for the “crisis pregnancy center,” I was already seeing an actual healthcare provider—who coincidentally just gave me a mandatory ultrasound.
- “That the man responsible for pregnancy is liable for providing assistance in supporting my child, if born, even if he has offered to pay for the abortion.” Maybe I’m naive, but I wasn’t expecting racist dog whistles on healthcare paperwork.
- “That I have the right to receive and review, free of charge, state-printed materials that describe the unborn child and list agencies that offer alternatives to abortion.” I will never understand why lawmakers think a person makes an appointment for an abortion without first considering whether they want an abortion. I am at Planned Parenthood because I want and need their services, not because I’m window shopping.
- “That I have the right to receive and review, free of charge, information on the availability of public and private agencies and services that provide birth control information including natural family planning information; information on services available for victims or individuals at risk of domestic abuse; information about legal protections for me and my child should I wish to oppose establishment of paternity or to terminate the father’s parental rights; and information on the availability of perinatal hospice.” Republican lawmakers, I would like to inform you that natural family planning is the reason I need an abortion right now.
And now, I wait a week. A week of nausea and exhaustion where each time I feel like puking is a reminder that people will think I’m a murderer. A week of waiting where I am acutely aware that this nausea means that what is inside of me could grow into a human – like my son did – or it could grow into a lump of miscarried cells that I would have to pass just as I did over two years ago. A week of feeling selfish, stupid, and every other message people in need of abortions have internalized as a result of decades of anti-choice stigma. This waiting period is not helping me make my decision. This waiting period is making me feel like shit – my body wracked by the early stages of a pregnancy I do not want, my head and heart weighed down by the shame that other people say I should feel.
It will be a long week.
-
There Is A Public Health Crisis in Dane County
By Liam Manjon
This was originally published on Free the 350 Bail Fund’s blog and is reprinted here with permission from the author, who is an organizer with Free the 350 Bail Fund and also a member of DSA. To contribute directly to Free the 350 Bail Fund and help free individuals incarcerated at the Dane County Jail visit Free the 350 Bail Fund’s website.
A public health crisis that was entirely avoidable had elected officials, judges and state department of corrections officials acted proactively to stop the spread of the deadly Covid-19 virus is now underway. After weeks of inaction by the sheriff, there are now myriad folks testing positive for the virus inside the Dane County jail. On Tuesday April 21 it was announced that 16 out of 22 people FROM A SINGLE pod have tested positive for COVID-19 and as a result the Dane County Sheriff has arranged for the National Guard to come into the jail and test everybody.
In the meantime, there are people who continue to exit and enter the jail, spreading the coronavirus to the broader community, which will result in the deaths of people in our neighborhoods due to the negligence of elected officials, judges, and state Department of Corrections officials. While increased testing being called for by the Sheriff in the jail is of course needed in order to be able to form cogent public policy to curb the spread of the deadly virus, the need to release people from the jails is imminent and pressing and should not be held off another day. COVID-19 could claim the lives of approximately 100,000 more people across the U.S. than current projections stipulate if jail populations are not dramatically and immediately reduced, according to a new epidemiological model released on April 26 by the ACLU and academic research partners. “The revolving doors of jails make them a tinderbox for COVID-19 spread within our communities.”
The lives of people in the community are at risk, yet elected officials, judges and Department of Corrections officials continue to drag their feet on what is a no-brainer of a solution – releasing people from the closed quarters of the jail, where social distancing is impossible. And indeed, elected officials, judges and Department of Corrections officials DO have the authority to release people from the jail. The Sheriff can place people on electronic monitoring, the Department of Corrections can release people’s probation/parole holds, the judges can change bails to signature bonds, the District Attorney can drop charges against people, the Dane County Board of Supervisors can reduce the operating budget of the jail, and Governor Evers has the power to commute the sentences of incarcerated people.
Although the death rate from the virus among the general population is extremely high, due to baked in racism in the systems of our white supremacist patriarchal capitalist society, it is EVEN HIGHER for Black, Indigenous and People of Color, which Dane County consistently, disproportionately, locks up in the Dane County jail. Therefore, it is a life and death proposition when considering whether or not to free people from the jail.
Folks who are incarcerated are essentially being served a death sentence by leaving them exposed to the virus without the ability to practice life saving social distancing measures and without being provided with sufficient Personal Protective Equipment (PPE). Although the death rate from the virus among the general population is extremely high, due to baked in racism in the systems of our white supremacist patriarchal capitalist society, it is EVEN HIGHER for Black, Indigenous and People of Color, which Dane County consistently, disproportionately, locks up in the Dane County jail. Therefore, it is a life and death proposition when considering whether or not to free people from the jail.
We have heard that one of the methods that the Sheriff has been utilizing to deal with the virus spreading in the jail is to lock people up in solitary confinement in an attempt to socially isolate them from the rest of the population. Solitary confinement is a form of torture and is considered a human rights abuse by the UN and other international bodies and is an unethical and ineffective tactic to employ during a pandemic.
Keeping people in close quarter cages during a pandemic is a cruel and unusual punishment, which is protected against in the eighth amendment of the constitution, which the elected officials are apparently ignoring.
More than 100 people have died across the countries in the jails and prisons so far, and the number is sure to rise should there continue to be no action taken.
The evidence is compelling and undeniable that we must free them all or be responsible for untold deaths. To put the icing on the cake, there is no proof that incarcerating people ACTUALLY reduces crime or violence in society, in fact there is evidence to the contrary, incarcerating people in jails and prisons increases crime and violence so the argument for keeping them in there is non existent.
Additionally, there is much precedent for freeing people. So far many countries including, Iran, Turkey, Ethiopia, Indonesia, India, Morocco and the UK have freed hundreds of thousands of people from their jails and prisons, recognizing the public health crisis that it poses. California, Washington and Ohio have, or are moving toward, freeing thousands, too, and many cities across the country have also moved to free people. So tell Sheriff David Mahoney, District Attorney Ismael Ozanne, the judges, the Dane County board of supervisors, the department of corrections and Governor Tony Evers to Free Them All NOW, before their inaction results in untold deaths of our loved ones and community members.
-

We Can’t Just “Bounce Back”
Reopening Requires Science
An Interview with Dr. Greg Gelembiuk by Dayna Long
Dr. Gelembiuk is a scientist in Madison. He is also a member of the Community Response Team, which seeks to reduce police use of force and to establish more oversight and accountability over police. He was appointed to the Police Department Policy & Procedure Review Ad Hoc Committee in 2019.
DL: Folks in Madison might be more familiar with your scientific approach to police accountability and reform than they are with your actual career as a scientist. I was hoping you might tell me a little bit about your background and your work and how it’s prepared you to follow the science around COVID-19?
GG: I’m a scientist. My doctorate is in Integrative Biology with a minor in Statistics. I worked in virology and oncology for about two decades, predominantly working on DNA tumor viruses. Then subsequently I’ve worked predominantly on evolution and genetics of invasive species. So I’ve got background in a wide variety of areas in the life sciences, including a great deal of background in virology.
DL: So I have no scientific background, like a lot of people. But at the start of this crisis I was checking the Department of Health Services website and Public Health Madison & Dane County website pretty much every day to look at the numbers. But I realized over time that they didn’t mean that much to me and I so want to hear from you. How useful are those numbers? Should they be taken with a grain of salt and is there something meaningful in those numbers that people can take away from them?
GG: They shouldn’t be taken with a grain of salt. However, they also represent a gross underestimate because of undertesting. The actual number of infections is probably roughly an order of magnitude higher than the confirmed number of infections. And undertesting also means that a lot of deaths due to Covid-19 are not being recorded.
I’ll also mention that I was highly critical of Public Health Madison & Dane County (PHM & DC) at the outset because back in mid-March, they seemed predominantly concerned with reassuring Madison. They had an online poster. The main feature of the poster was a big fat zero, that we had zero cases here, and then accompanying text saying that we were at low risk. This was at a point when I was pressing for immediate enactment of social distancing policies and in my view, PHM & DC was entirely failing to fill its proper role at that point. Any epidemiologist recognized that we were about to be hit and that there probably already was community spread going on here. And yet that was not the messaging that PHM & DC was providing.
DL: Have your feelings about folks going to those websites changed at all? Is it useful for me as a person living in Madison to look at the number of cases or the number of deaths every day?
GG: Deaths are a lagging indicator. If you track the trend of cases that will tell you something. Now again I’ll note that we’re grossly undertesting and constraints on test availability will distort the curve. But still the trajectory of the curve will give you some important information.
DL: My understanding as a person following the news was that a lot of people will not even know that they have COVID-19. It seems like a large number of people may not have symptoms at all. But what you’ve been saying is that that’s maybe not the case and that over time more people have had symptoms than was initially reported. What’s your understanding of that picture at this point?
GG: With COVID-19, some fraction of people will be true asymptomatics — they’ll never experience symptoms. Now those people may actually have, for example, lung damage if you look with a CT scan, but they won’t be feeling any symptoms yet they’re contributing to transmission. There’s another large segment of people who will be pre-symptomatic, will be transmitting the virus, but will not yet be experiencing symptoms. So for example, the World Health Organization (WHO) noted that looking at numbers from China that people who were tested and were found to be positive and at the time were asymptomatic, about three-quarters of them went on to develop symptoms.
The fraction of true asymptomatics who will never develop symptoms is not yet well established. It’s somewhere probably in the range between 7% and 40%. Right now my ballpark guess would be maybe about a quarter (25%). But there are a lot of other people who are pre-symptomatic, so temporarily not experiencing symptoms but then will go on to develop them.
The most important take home from all that is that much of the transmission, about half, is from people who, at the time, are not experiencing symptoms. Right now, all of our testing is of people who are experiencing symptoms and usually testing is only available to those who are experiencing severe symptoms. That’s a problem. Because if you don’t test asymptomatics – if you don’t test in a ubiquitous manner – testing all people at pretty high frequency – then you’re not going to be able to suppress the virus.
DL: Right, because you can’t track the spread then. That makes sense.
GG: Right. There’s some very good public health plans that are coming out. One from Paul Romer, also one from the Rockefeller Foundation, there are good plans for suppressing it with a combination of ubiquitous testing and intensive contact tracing. That’s where we have to go. That’s what South Korea did, very successfully. That’s what we’ve failed to do so far.
Now, given how widely it’s spread, there needs to be some kind of technological innovation to be able to test that large a number. That innovation is already well under way. There’s a protocol called SwabSeq that would allow really large, population-scale testing. One lab tech using that protocol could test a thousand samples a day. If you actually use an automated system, like robotic systems, you could test a hundred thousand in a day and that’s just with one machine operated by one tech. I’ve been arguing that this needs to be implemented ASAP and that it would be good to have a pilot program here in Madison. You could test, for example, first responders and healthcare workers since they’re the people who are most likely to transmit if they’re infected, as an initial pilot. It would also be good to include all staff and residents of nursing homes, given their vulnerability. Other methods such as testing using a surface plasmon resonance approach would take slightly longer to work out and deploy at scale, but would allow for cheap, quick testing of everyone with results in only a few minutes.
DL: Is science also susceptible to pressure by politicians and businesses and their interests? What are some examples you’ve seen of that sort of thing during the COVID-19 crisis?
GG: Oh yeah. Science is, unfortunately, susceptible to this. A perfect example is the recent, terrible quality studies that have come out from a group at Stanford. That includes a study of seroprevalence (the level of a pathogen in a population, as measured in blood serum) in Santa Clara County and a study of seroprevalence in Los Angeles County. This group is doing incredibly poor science. If you look at their paper on Santa Clara County, there were simple math errors. There were errors in design, it wasn’t randomized. There were major problems with how they were recruiting people. People who believed they’d been exposed to COVID-19 were much more likely to enter this study. And they lied to recruit test subjects and violated informed consent requirements. Their confidence intervals were just inherently wrong. They were using technology that has not been adequately vetted and that is known to give a high false positive rate.
A lot of people seem to misunderstand the logic of epidemiology. The social distancing we’re doing now – all that does is temporarily freezes in place the situation where infection has not swept through the population. That buys us time. It doesn’t resolve the situation.
So what they’re putting out is a hot mess. And yet it got a lot of coverage. It got an article in the New York Times where the reporter failed to interview any of the numerous scientists who were pointing out that this study was actually complete trash. [Their study] was widely publicized by conservative media, claiming that Covid-19 was no worse than the flu. Now one of the interesting things I’ll note is that when the same group released the initial tech report that described their Los Angeles study, the place where it was first published was the conservative GOP blog RedState. Now it’s very telling that these scientists chose to first release their publication there. What you’re seeing in some cases like this is far outside the norms of how science is supposed to operate.
So you do have a problem with political pressure affecting the science and the public’s understanding of the science. You can see what’s happening with the CDC. I have enormous respect for Dr. Fauci, but you can tell that he has to toe the line to a certain extent and he’s not able to speak entirely freely, to the point where he has had to basically fall on his sword at times. Meanwhile the CDC had been, to a large extent, gutted by the Trump Administration driving out scientists by budget cuts from the current administration. The quality of the work that the CDC has done recently is far inferior to the quality of the work it’s historically done. So yeah, political pressures can have an enormous impact – an unfortunate impact – on the science.
DL: Given the potential for science to be distorted for political means, one of my concerns for myself and for other workers is understanding when it’s actually safe to go back to work, because our priorities, like staying healthy and safe, aren’t the same as our employers’ priorities. We’re already seeing a lot of pressure from the Republican party in our state to reopen. Do you have any advice for folks about evaluating the situation for themselves? What things need to happen before we reach a point where that’s a realistic and safe thing for non-essential workers?
GG: The only way that that could happen is with a program of ubiquitous testing, intensive contact tracing, and then quarantine. Without that, it’s not going to be safe to go back to work. There’s going to hopefully be a vaccine but the earliest I would expect a vaccine availability is maybe eighteen months.
A lot of people seem to misunderstand the logic of epidemiology. The social distancing we’re doing now – all that does is temporarily freezes in place the situation where infection has not swept through the population. That buys us time to do other things like testing, contact tracing, developing better therapy, developing a vaccine. That buys us time. It doesn’t resolve the situation.
As soon as social distancing is relaxed, the epidemic which has basically been frozen in place at a lower number, will then again take off in an exponential fashion sweeping through the population. There seems to be this widespread misunderstanding that as numbers have plateaued or if numbers are going down, then you can reopen. From an epidemiological perspective, that is wrong. That makes absolutely no sense. You cannot safely reopen, you cannot safely resume your old practices and your usual work conventions until you’ve really suppressed the virus.
Right now the only practical means for doing that in the short term is ubiquitous testing and extensive contact tracing.
DL: And we don’t have that in Wisconsin, of course.
GG: No. In fact, it’s not happening anywhere in the US. It’s not close to happening anywhere in the US. For this to happen properly in the US we will need roughly around thirty million tests done a day. That’s possible with the technology that I was mentioning earlier, with a logistical system set in place to really collect and process the samples. So basically you need a situation where, for example, everybody is spitting in a tube and sending it to a test center and tests are being run on [the samples] and you do that, maybe, every week or so.
DL: Have you taken a look at the Badger Bounce Back Plan? What do you think of that?
GG: Okay, one – I feel some sympathy for the Evers administration given the pressure they’re under, given that the Republicans are now appealing the Stay At Home order to the State Supreme Court. However, the plan as written is garbage. If you look at the plan it does not follow the logic of epidemiology at all. The gating criteria the state is using to determine if we can begin reopening under the plan is a decrease across a fourteen day period in the number of new cases. That’s insane.
If you’re at a very high level and you decrease for fourteen days, you’re still at a very high level off the ground. It’s basically equivalent to someone who jumped out of a plane with a parachute, the parachute has slowed their fall, and then they say, “Oh. For a period of time my fall has been slower so I’ll take the parachute off now.” It’s crazy.
You know, another criteria in the plan is that there’s been some progress made on the amount of testing. That means nothing. What does it mean to make some progress on the amount of testing? You do a dozen more tests in a week and that’s criteria for reopening? The plan makes no scientific sense. Any reopening plan should be using the World Health Organization criteria, which are well thought out and fully scientifically defensible.
I’ll mention one other thing. I’ve written correspondence to Evers office. There’s been no reply. There was a letter that I and ten other scientists from the University of Wisconsin, predominantly professors, wrote to the Governor’s office – and sent it to his Chief of Staff as well as the staff for Mandela Barnes. And there’s been zero reply. Among other things, the letter pointed to what needed to be done with testing and also suggested that Evers administration should tap scientists, including UW scientists, to set up a scientific advisory panel, which is really needed, especially if you look at the Badger Bounce Back Plan.
I feel sympathy for Evers and want to see substantial support for Evers given the pressure from Republicans. But the only way to deal with this properly is to actually follow the science.
DL: What developments in the science around COVID-19 are you looking for? Are there sources that you feel good about that lay people could also follow along with?
GG: Scientific developments that I’m looking at: improvements in therapies; progress on potential vaccines, though again, that won’t come out for a very long time; looking at improvements in modeling that can provide more accurate projections. Clinically, improvements in testing methodologies, new developments in serology testing. Those are a few of the things that I’m tracking and that people should keep an eye out for.
There are a lot of good sources out there. I would recommend people follow Carl T Bergstrom on Twitter. He’s often got very good analysis. And there are a lot of other scientists on Twitter who are providing good, meaningful analysis: Natalie Dean, Jennifer Nuzzo, Eric Topol, and Mark Lipsitch are some examples. As far as online magazines, the journal Nature is good; Science Magazine is good. There’s a lot of stuff that people can access that really can speak to a mass audience and that provide good analysis and helps people understand what’s going on.
Carl Bergstrom especially cuts through the bullshit. And there’s a lot of bullshit out there right now. Like the IHME model, for example, is trash. Yet that has been treated as the most influential model in the US. But it’s fundamentally flawed, it’s not really an epidemiological model at all. It’s based on assumptions that are known to be totally incorrect. Its predictions – on expected number of deaths, on dates to expect peaks, etc. – have consistently been very wrong in both the U.S. and other nations. No-one should be using or referencing it. And Bergstrom has provided very trenchant analysis of the flaws in that model, as well as analysis of a lot of other relevant science.
Red Madison is grateful to Dr. Gelembiuk for his contributions and encourages more scientists and healthcare professionals to share their knowledge about COVID-19 and help workers navigate pressure to reopen in unsafe conditions. If you are interested in sharing your perspective with Red Madison, you can send us an email at redmadison (at) googlegroups (dot) com.